Written By: Dr. Gagandeep Singh
Medically Reviewed By: Dr. Gagandeep Singh, MBBS
Last Updated: 1 April 2026
Most patients are told they have ‘high sugar’ — but the deeper problem often starts years earlier with insulin resistance. Long before your fasting blood sugar crosses the diagnostic line for diabetes, your body may already be producing two or three times the normal amount of insulin just to keep glucose levels in check. This silent metabolic strain is one of the most under-recognised drivers of type 2 diabetes, and it rarely shows up on a standard blood test.
In our clinic, we routinely see patients whose reports say ‘everything is normal’ — yet their waistline, energy levels, and post-meal crashes tell a very different story. This article explains what insulin resistance actually means, why it develops, how to recognise it early, and what you can do about it.
| ✓ Key Takeaways |
| • Insulin resistance means your cells no longer respond efficiently to insulin, forcing the pancreas to produce more of it to keep blood sugar in range. |
| • You can have insulin resistance for years with completely normal fasting blood sugar — the standard test most people rely on. |
| • Common early signs include stubborn belly fat, fatigue after meals, skin darkening (acanthosis nigricans), and difficulty losing weight despite effort. |
| • A fasting insulin test or HOMA-IR calculation can detect insulin resistance far earlier than fasting glucose or HbA1c alone. |
| • Insulin resistance is the root cause behind most cases of type 2 diabetes, and it is often improvable with targeted dietary changes, physical activity, sleep, and medical supervision. |
| • Indian populations are at higher genetic and dietary risk — ICMR data shows diabetes prevalence in India has risen to over 11% of the adult population. |
A Simple Explanation: Glucose, Insulin, and Why Cells Stop Responding Well
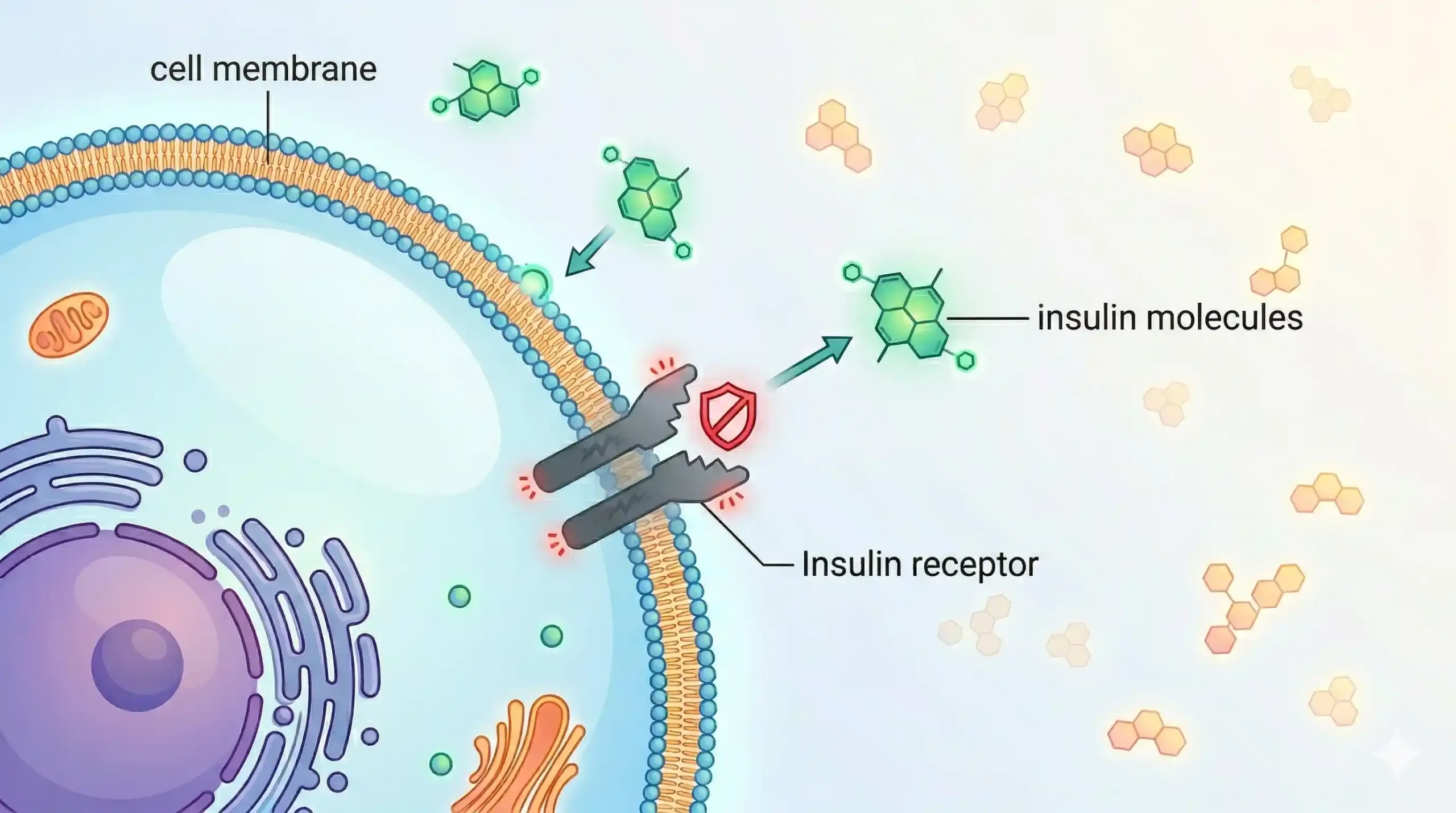
Insulin resistance is a condition in which your body’s cells — particularly in the muscles, liver, and fat tissue — stop responding effectively to insulin, the hormone responsible for moving glucose from your blood into your cells for energy. When this happens, your pancreas compensates by producing more and more insulin to maintain normal blood sugar levels.
Think of it this way: insulin is the key, and your cell receptors are the lock. In a healthy body, insulin fits smoothly into the lock and opens the door for glucose to enter. In insulin resistance, the lock becomes stiff. The key still works, but you need to turn it harder — and eventually, even turning harder may not be enough.
This compensation can go on silently for years. Your blood sugar may test ‘normal’ because your pancreas is working overtime behind the scenes. But the excess insulin circulating in your body (a state called hyperinsulinaemia) is already causing metabolic damage — driving fat storage, increasing inflammation, and raising triglyceride levels.
At Redial Clinic in Green Park, New Delhi, we frequently see patients whose fasting glucose sits at a reassuring 90–95 mg/dL, while their fasting insulin is already 18–25 µIU/mL — well above optimal. The glucose looks fine; the insulin tells you the engine is already straining.
How Insulin Resistance Progresses Into Prediabetes and Type 2 Diabetes
 Insulin resistance is not a sudden event — it is a gradual metabolic shift that can take 5–15 years to progress from early compensated resistance to frank type 2 diabetes. Understanding this timeline is critical because it shows just how many opportunities exist for early intervention.
Insulin resistance is not a sudden event — it is a gradual metabolic shift that can take 5–15 years to progress from early compensated resistance to frank type 2 diabetes. Understanding this timeline is critical because it shows just how many opportunities exist for early intervention.
The typical progression looks like this:
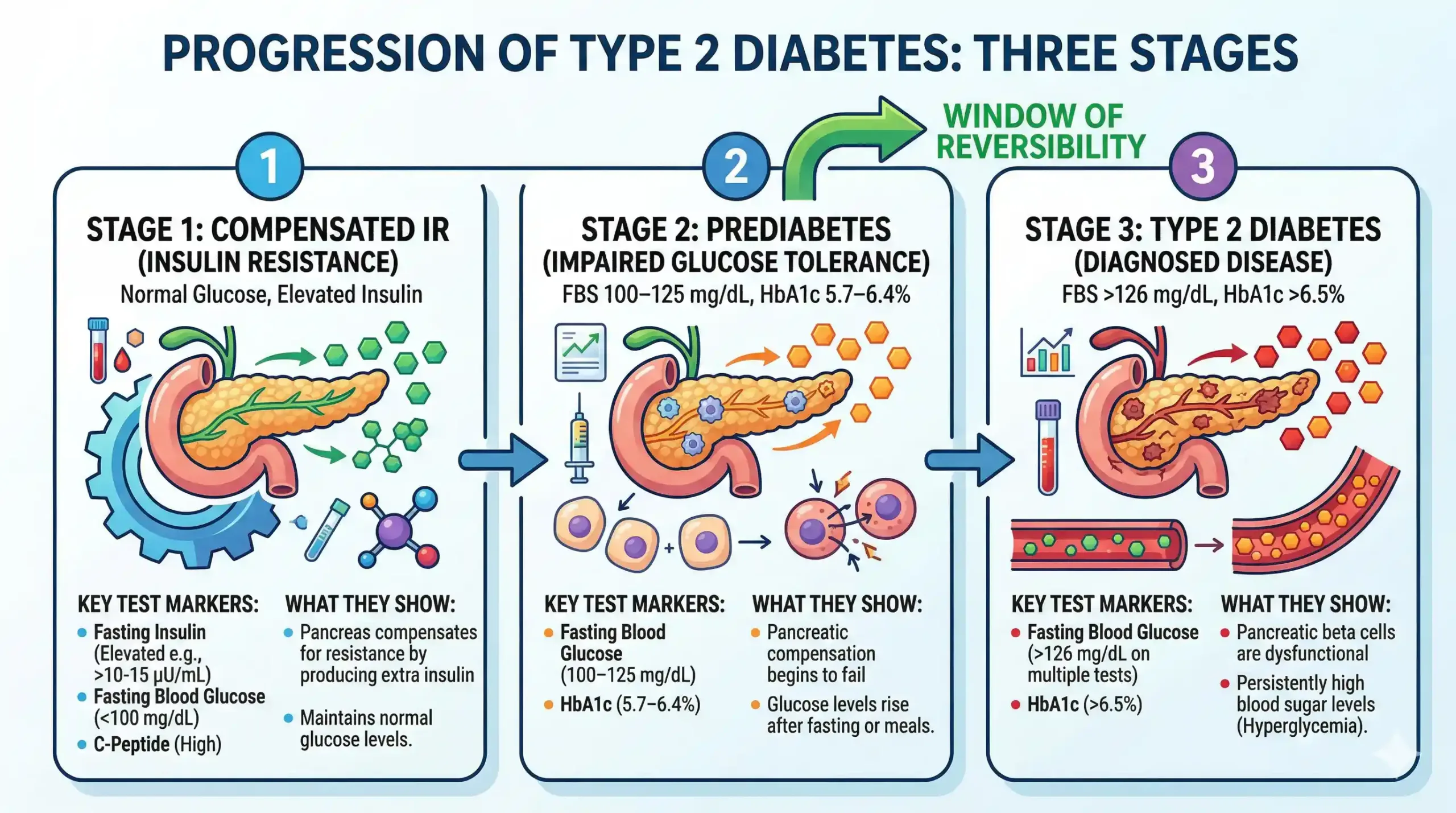
Stage 1 — Compensated insulin resistance: Cells begin to resist insulin, but the pancreas increases insulin production to compensate. Blood sugar remains normal. Most standard tests show nothing abnormal at this stage. Only fasting insulin or HOMA-IR would reveal the problem.
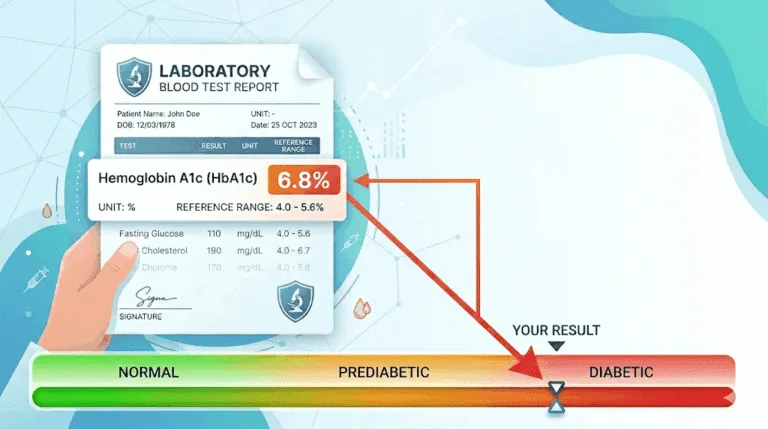
Stage 2 — Prediabetes: The pancreas can no longer fully compensate. Fasting blood sugar rises to 100–125 mg/dL, or HbA1c climbs to 5.7–6.4%. Post-meal glucose spikes become more pronounced. This is the stage where most people first receive a warning — but many dismiss it as ‘borderline’.
Stage 3 — Type 2 diabetes: Pancreatic beta cells become exhausted and can no longer produce enough insulin. Fasting blood sugar exceeds 126 mg/dL, HbA1c crosses 6.5%, and the clinical diagnosis is made.
A landmark study published in The Lancet found that the progression from prediabetes to diabetes occurs at a rate of approximately 5–10% per year, depending on risk factors. But crucially, studies like the Diabetes Prevention Program (DPP) have shown that lifestyle interventions can reduce this progression by up to 58%.
Common Signs That Suggest Insulin Resistance
The most common signs of insulin resistance include stubborn belly fat, fatigue after meals, sugar cravings, difficulty losing weight, and darkened skin patches — particularly around the neck, armpits, or groin (a condition called acanthosis nigricans). However, many people with insulin resistance have no obvious symptoms at all, which is why it often goes undetected.
Signs to watch for:
- Increasing waist circumference — especially above 90 cm in Indian men or 80 cm in Indian women (ICMR thresholds, which are lower than Western cut-offs)
- Post-meal fatigue or brain fog — a common complaint we hear at Redial Clinic, often dismissed as ‘normal tiredness’
- Difficulty losing weight despite consistent diet and exercise effort
- Skin tags (small, soft growths) on the neck or armpits
- Darkened skin folds (acanthosis nigricans)
- Elevated triglycerides or low HDL cholesterol on a lipid panel
- PCOS in women — polycystic ovary syndrome is strongly linked to insulin resistance
- Strong cravings for carbohydrate-heavy foods, especially after meals
In our practice, patients with insulin resistance often present with fatigue and post-meal crashes long before their fasting sugar crosses the diagnostic line. When we add fasting insulin to their workup, the picture changes completely.
Why Normal Fasting Sugar Can Miss the Problem Early
Fasting blood sugar is one of the last markers to become abnormal in the insulin resistance timeline — by the time it rises above 100 mg/dL, the underlying metabolic dysfunction may have been developing for years. This is why relying on fasting glucose alone gives many patients a false sense of security.
The reason is straightforward: your pancreas works hard to keep fasting glucose within range by producing extra insulin. As long as it succeeds, the glucose number looks normal. The problem is that nobody checked how much insulin it took to achieve that number.
This is where a fasting insulin test becomes valuable. A fasting glucose of 92 mg/dL with a fasting insulin of 5 µIU/mL tells a very different metabolic story from a fasting glucose of 92 mg/dL with a fasting insulin of 22 µIU/mL. The glucose is identical; the insulin load is vastly different.
Similarly, post-meal glucose testing or a continuous glucose monitor (CGM) can reveal glucose spikes after meals that a single fasting test completely misses. For a deeper explanation of why fasting sugar alone is insufficient, see our detailed article on why checking only fasting blood sugar is not enough.
What Causes Insulin Resistance
Insulin resistance develops from a combination of genetic predisposition, excess body fat (especially visceral fat around the organs), physical inactivity, poor sleep, chronic stress, and dietary patterns high in refined carbohydrates and ultra-processed foods. No single factor causes it alone — it is the accumulation of multiple metabolic stressors over time.
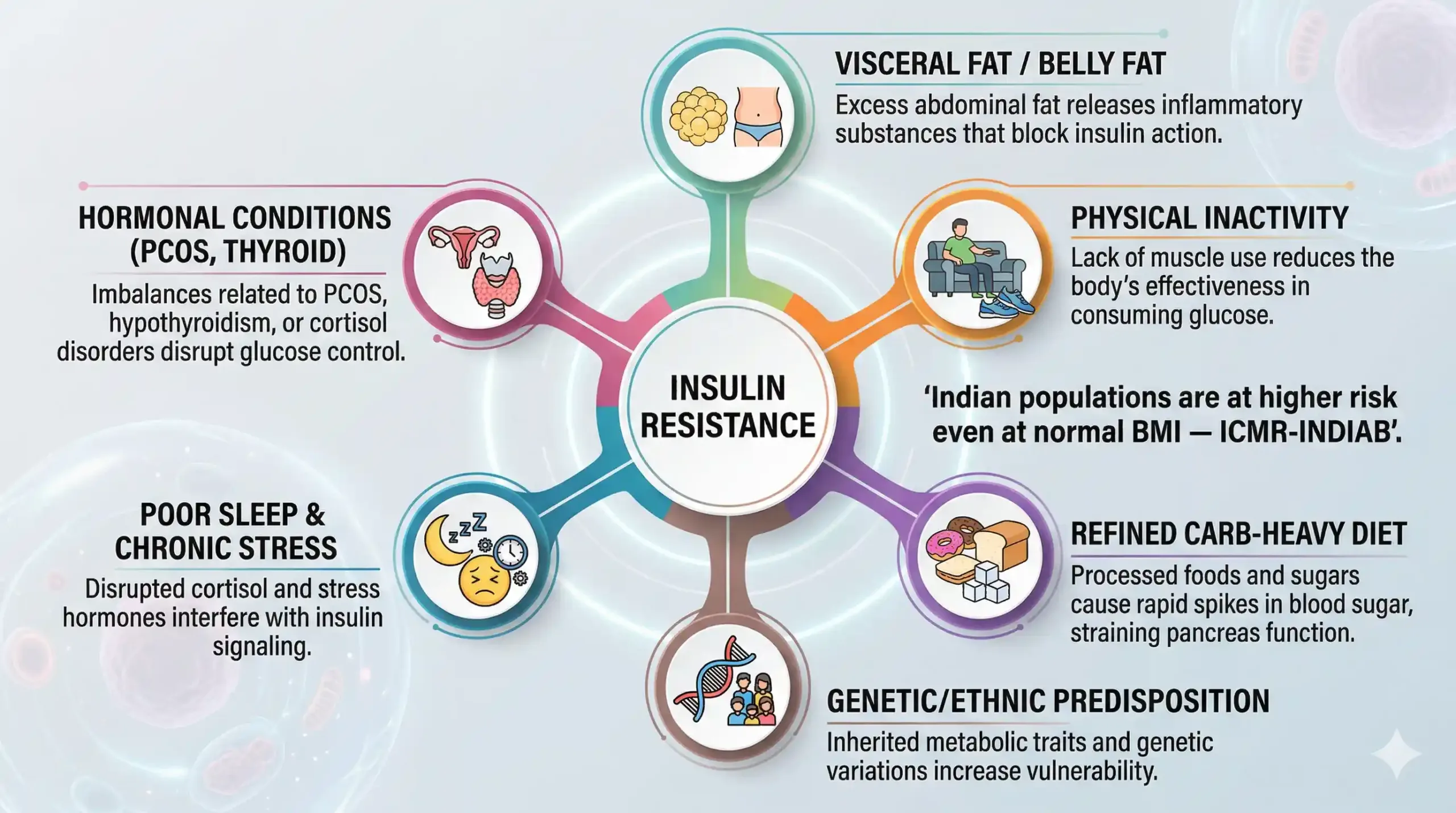
The major contributing factors include:
Excess visceral fat. Fat stored around the abdomen and internal organs is metabolically active — it releases inflammatory compounds (cytokines) that interfere with insulin signalling. Research published in Diabetes Care has consistently linked visceral adiposity to insulin resistance independent of total body weight. This is particularly relevant for Indian populations, who tend to accumulate visceral fat at lower BMI levels than Western populations — a phenomenon sometimes called the ‘thin-fat Indian’ phenotype.
Physical inactivity. Skeletal muscle is the largest consumer of glucose in the body. When muscles are inactive, they become less responsive to insulin. Regular physical activity, particularly resistance training and post-meal walks, improves insulin sensitivity through mechanisms that are independent of weight loss.
Dietary patterns. Diets high in refined carbohydrates, added sugars, and ultra-processed foods drive repeated glucose and insulin spikes. In the Indian context, meals that are heavily carbohydrate-weighted — a plate of white rice with a small serving of dal, or multiple rotis with minimal protein — can contribute to sustained hyperinsulinaemia over time. This is not about eliminating carbohydrates; it is about rebalancing the plate with adequate protein, healthy fats, and fibre. For practical guidance, see our article on the best Indian diet for diabetes reversal.
Genetics and ethnicity. South Asians have a higher genetic predisposition to insulin resistance compared to many other ethnic groups. ICMR-INDIAB study data shows that India’s diabetes prevalence has climbed to over 11% of the adult population, with an additional 15% classified as prediabetic. The combination of genetic susceptibility and rapid dietary urbanisation has created what researchers call a ‘diabetes epidemic in a non-obese population’.
Sleep deprivation and stress. Even a few nights of poor sleep can measurably reduce insulin sensitivity. Chronic stress raises cortisol, which in turn promotes both visceral fat accumulation and insulin resistance. These are often overlooked contributors that we assess routinely at Redial Clinic as part of a metabolic workup.
Hormonal conditions. PCOS, hypothyroidism, and Cushing’s syndrome can all worsen or trigger insulin resistance. Women with PCOS should be routinely screened for insulin resistance as part of their metabolic evaluation.
How to Improve Insulin Resistance Naturally and Medically
Insulin resistance can often be significantly improved — and in many cases functionally reversed — through a combination of dietary restructuring, regular physical activity, sleep optimisation, stress management, and, where indicated, targeted medication. The key is early, sustained action rather than short-term fixes.
Evidence-based strategies that make the most difference:
1. Restructure your meals around protein, fibre, and healthy fats. Rather than eliminating food groups, the goal is to reduce the glycaemic load of each meal. Start every meal with protein and vegetables before eating carbohydrates. In practical Indian terms, this means prioritising dal, paneer, eggs, curd, and sabzi before roti or rice — not after. For more on this approach, read our article on the most effective diet for diabetes reversal.
2. Move consistently — especially after meals. A 15–20 minute walk after lunch or dinner can reduce post-meal glucose spikes by 20–30%. Resistance training (bodyweight exercises, weights, or resistance bands) is particularly effective because it builds muscle tissue, which is the body’s largest glucose sink. The American Diabetes Association recommends at least 150 minutes of moderate-intensity activity per week.
3. Prioritise sleep. Studies show that even 4–5 nights of restricted sleep (fewer than 6 hours) can reduce insulin sensitivity by up to 25%. Aim for 7–8 hours of consistent, quality sleep.
4. Manage stress actively. Chronic stress elevates cortisol, which directly promotes insulin resistance and visceral fat accumulation. Techniques like deep breathing, regular physical activity, and structured routines help lower cortisol levels over time.
5. Medication when appropriate. Metformin remains the most widely prescribed medication for insulin resistance and early type 2 diabetes. It works primarily by reducing hepatic glucose output and improving insulin sensitivity. Newer agents like GLP-1 receptor agonists and SGLT2 inhibitors may also be used in specific clinical scenarios. Medication decisions should always be made in consultation with your physician.
The Diabetes Prevention Program (DPP), one of the largest clinical trials on this topic, demonstrated that lifestyle modification (diet and exercise resulting in ~7% body weight loss) reduced the progression from prediabetes to diabetes by 58% — even more effective than metformin alone (31% reduction). For Indian populations, the Indian Diabetes Prevention Programme (IDPP-1) showed similar results, confirming that lifestyle intervention is effective even in a South Asian population with a higher baseline metabolic risk.
When to Get Evaluated
You should consider a metabolic evaluation for insulin resistance if you have a family history of type 2 diabetes, carry excess weight around the midsection, have been diagnosed with PCOS or fatty liver, or notice signs like persistent fatigue, post-meal crashes, or difficulty losing weight. Early detection gives you the widest window for reversal.
A thorough insulin resistance evaluation should include:
- Fasting insulin — not part of routine blood work in most labs, but essential for early detection
- HOMA-IR calculation — derived from fasting glucose and fasting insulin; a score above 2.0–2.5 suggests resistance
- HbA1c — a 3-month average of blood sugar
- Fasting and post-meal glucose — ideally both, not just fasting
- Lipid profile — particularly triglycerides and HDL ratio
- Waist circumference — using ICMR cut-offs: >90 cm for men, >80 cm for women
At Redial Clinic’s diabetes reversal programme, one of the first things we assess in a metabolic workup is fasting insulin alongside standard markers. This single addition often changes the clinical picture entirely — revealing resistance that would otherwise go undetected for years.
Frequently Asked Questions
1. Can you have insulin resistance with normal blood sugar?
Yes. Insulin resistance often exists for years with completely normal fasting blood sugar. This happens because the pancreas compensates by producing extra insulin to keep glucose in range. A fasting insulin test or HOMA-IR calculation can detect resistance at this early stage, even when standard glucose tests appear normal. This is why experts increasingly recommend fasting insulin as part of metabolic screening, particularly for individuals with risk factors.
2. Is insulin resistance reversible?
In many cases, yes. Insulin resistance can be significantly improved and often functionally reversed through dietary changes, regular exercise, weight management, and improved sleep. The Diabetes Prevention Program trial showed a 58% reduction in diabetes progression with lifestyle changes alone. However, the degree of improvement varies depending on how long the resistance has been present, genetic factors, and how consistently interventions are maintained. Early detection gives the best chance of meaningful reversal.
3. What foods worsen insulin resistance?
Foods that cause rapid and repeated blood sugar spikes tend to worsen insulin resistance over time. These include refined carbohydrates (white bread, maida-based products, instant noodles), sugary beverages (packaged juices, sweetened chai, soft drinks), ultra-processed snacks, and meals that are heavily carbohydrate-weighted with minimal protein or fibre. In the Indian dietary context, large portions of white rice or multiple rotis without adequate dal, sabzi, or protein are a common pattern that contributes to sustained hyperinsulinaemia.
4. Which test is best for insulin resistance?
The most practical clinical test for insulin resistance is the fasting insulin level combined with fasting glucose to calculate HOMA-IR (Homeostatic Model Assessment of Insulin Resistance). A HOMA-IR score above 2.0–2.5 generally indicates insulin resistance. While the euglycaemic insulin clamp is considered the gold standard in research, it is not used in routine clinical practice. For ongoing monitoring, HbA1c, post-meal glucose, and lipid ratios provide complementary information. Discuss adding fasting insulin to your next blood test with your doctor.
If your fasting sugar has been ‘normal’ but you still feel something is off — persistent fatigue, stubborn belly fat, post-meal crashes, or a family history of diabetes — a comprehensive metabolic workup can reveal what standard tests miss.
Book a metabolic assessment with our team at Redial Clinic, Green Park Extension, New Delhi. We include fasting insulin, HOMA-IR, and a full metabolic risk profile as standard — because catching insulin resistance early is the single most effective way to prevent type 2 diabetes.
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before making changes to your diet, exercise, medication, or treatment plan.
References
1. Tabák AG et al., “Prediabetes: a high-risk state for diabetes development,” Lancet, 2012. https://doi.org/10.1016/S0140-6736(12)60283-9
2. Knowler WC et al., “Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin,” New England Journal of Medicine, 2002. https://doi.org/10.1056/NEJMoa012512
3. Ramachandran A et al., “The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1),” Diabetologia, 2006. https://doi.org/10.1007/s00125-005-0097-z
4. Anjana RM et al., “Prevalence of diabetes and prediabetes in 15 states of India: results from the ICMR-INDIAB population-based cross-sectional study,” Lancet Diabetes & Endocrinology, 2017. https://doi.org/10.1016/S2213-8587(17)30174-2
5. American Diabetes Association, “Standards of Care in Diabetes — 2024,” Diabetes Care, 2024. https://doi.org/10.2337/dc24-SINT
6. ICMR Guidelines for Management of Type 2 Diabetes, Indian Council of Medical Research, 2018. https://main.icmr.nic.in/sites/default/files/guidelines/ICMR_GuidelinesType2diabetes2018_0.pdf
7. Yajnik CS, “The insulin resistance epidemic in India: fetal origins, later life consequences, and practical implications,” Nutrition, 2001. https://doi.org/10.1016/S0899-9007(01)00509-6