
Written By: Dr. Gagandeep Singh | Medically Reviewed By: Dr. Gagandeep Singh, MBBS |
Last Updated: 13/04/2026
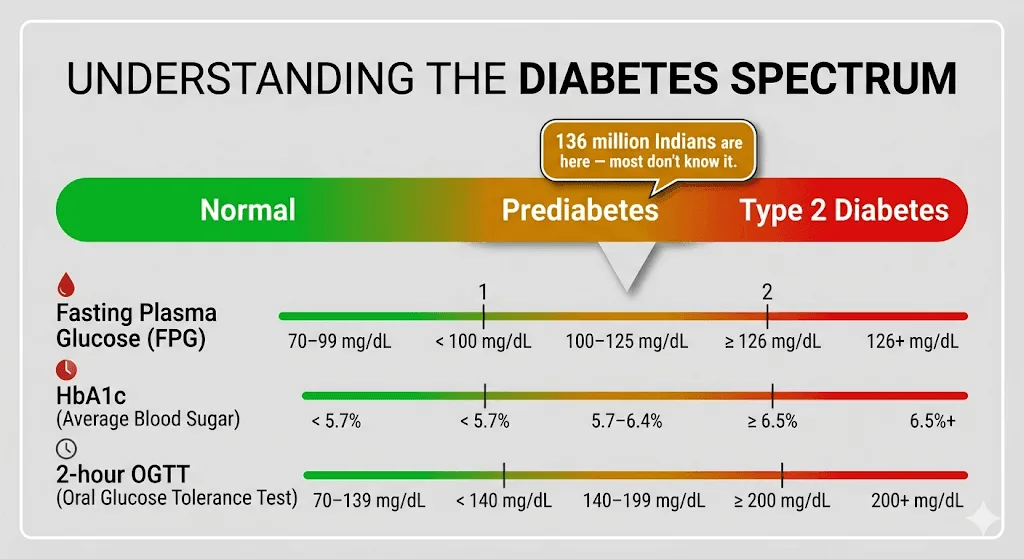
Prediabetes is often treated like a polite warning — something a patient hears, nods at, and files away alongside advice about flossing more. In reality, it is closer to the last quiet knock before a much louder problem arrives. An estimated 136 million Indians now live with prediabetes, according to recent ICMR-INDIAB data — and the vast majority do not know it.
At Redial Clinic in Green Park, New Delhi, we see patients every week whose lab reports say “borderline” or “slightly elevated” — phrases that sound reassuring but often mask a metabolic shift that has been developing silently for years. The good news? Prediabetes is one of the most responsive conditions in medicine. Caught early enough, it can genuinely be reversed — not with miracle supplements or crash diets, but with structured, sustained lifestyle changes backed by some of the strongest clinical evidence in preventive medicine.
This article explains what prediabetes actually means, why it develops, what the evidence says about reversing it, and what practical steps make the biggest difference — with Indian context, Indian dietary patterns, and realistic timelines.
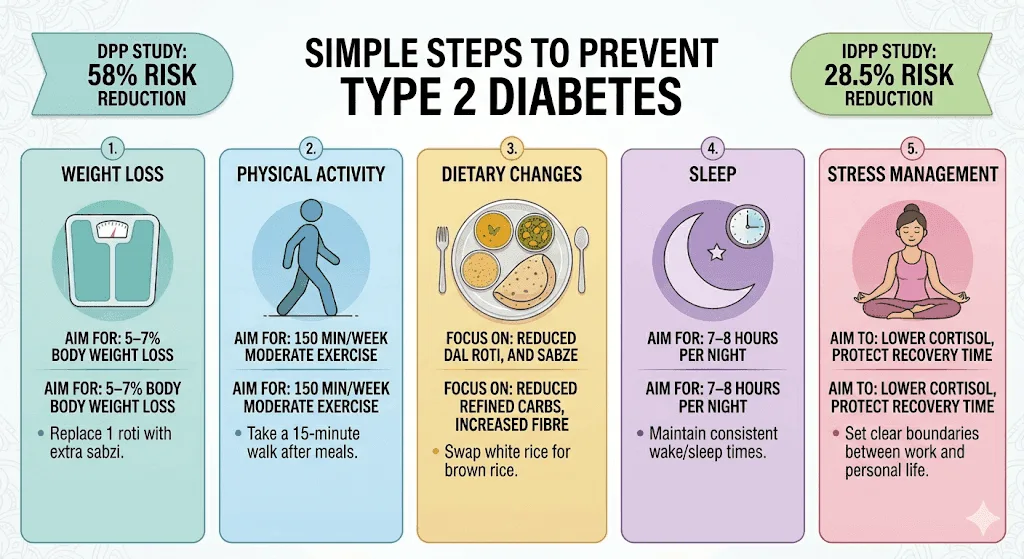
| Key Takeaways Prediabetes means your blood sugar is above normal but below the diabetes threshold — an HbA1c between 5.7% and 6.4%, or fasting glucose between 100 and 125 mg/dL. The landmark Diabetes Prevention Program (DPP) showed that lifestyle changes reduced the risk of progressing to type 2 diabetes by 58% — more effective than medication alone. The Indian Diabetes Prevention Programme (IDPP-1) confirmed that even modest lifestyle changes reduced diabetes progression by 28.5% in an Indian population that was younger and leaner than Western study cohorts. Reversal is most effective when caught early. Losing 5–7% of body weight and getting 150 minutes of moderate activity per week are the two most evidence-backed interventions. Prediabetes can affect lean individuals too — especially South Asians, who develop insulin resistance at lower BMIs than Western populations. Medication (typically metformin) may be appropriate when lifestyle changes alone are insufficient, particularly for patients with both impaired fasting glucose and impaired glucose tolerance. |
What Prediabetes Means in Plain English
Prediabetes is the stage where blood sugar levels are higher than normal but have not yet crossed the diagnostic threshold for type 2 diabetes. It is not a separate disease — it is an early phase of the same metabolic process that leads to diabetes if left unaddressed. Think of it as the body’s way of signalling that its glucose-regulating system is under strain.
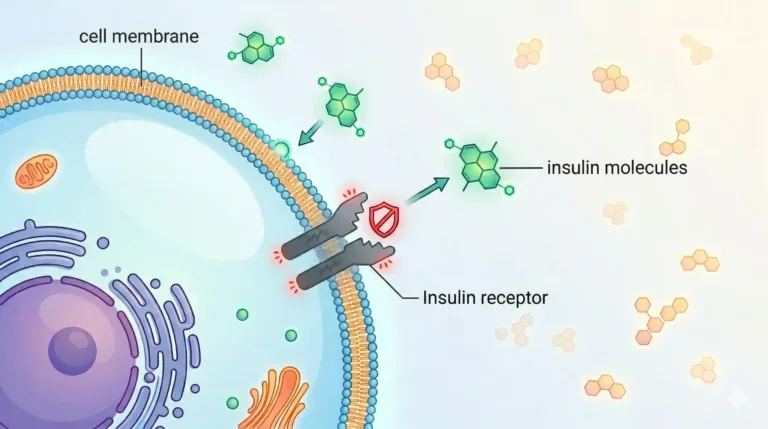
Under normal circumstances, when you eat, your body breaks carbohydrates down into glucose. The pancreas releases insulin, which helps cells absorb that glucose for energy. In prediabetes, cells begin responding less efficiently to insulin — a phenomenon called insulin resistance. The pancreas compensates by producing more insulin, but over time, it struggles to keep up. Blood sugar starts creeping upward — not dramatically, but enough to cause quiet damage to blood vessels, nerves, and organs.
What makes prediabetes deceptive is the absence of obvious symptoms. Most people feel perfectly fine. There is no pain, no dramatic weight change, no sudden thirst. In our clinic, patients are often surprised when a routine blood test reveals the problem — they came in for something else entirely.
Clinically, prediabetes is defined by any of the following:
| Test | Normal | Prediabetes |
| Fasting Plasma Glucose | Below 100 mg/dL | 100–125 mg/dL |
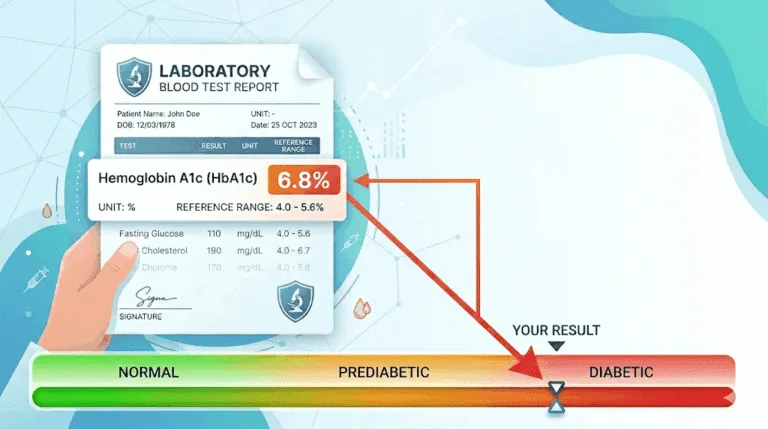
| HbA1c | Below 5.7% | 5.7%–6.4% |
| 2-Hour OGTT | Below 140 mg/dL | 140–199 mg/dL |
If any one of these markers falls in the prediabetic range, it warrants attention. If two or more are elevated, the metabolic shift is typically more advanced.
Can Prediabetes Really Be Reversed?
Yes — prediabetes can be reversed, and the clinical evidence supporting this is among the strongest in preventive medicine. Reversal means returning blood sugar markers to the normal range and restoring healthy insulin sensitivity, not merely slowing down the progression toward diabetes.
The most influential evidence comes from the US Diabetes Prevention Program (DPP), a landmark trial involving over 3,200 adults with prediabetes. Participants who followed a structured lifestyle intervention — targeting 7% body weight loss and 150 minutes of moderate physical activity per week — reduced their risk of developing type 2 diabetes by 58% compared with the placebo group. Among participants aged 60 and older, the reduction was even higher at 71%. These effects persisted: a 21-year follow-up showed sustained reductions in cumulative diabetes incidence.
Crucially for Indian patients, the Indian Diabetes Prevention Programme (IDPP-1) tested whether these findings applied to South Asian populations — who tend to develop insulin resistance at lower BMIs and younger ages. The study randomised 531 participants with impaired glucose tolerance in Chennai. Lifestyle modification alone reduced diabetes progression by 28.5% over three years. While the absolute reduction was lower than the DPP, it confirmed that lifestyle changes work in Indian populations, even at lower body weights.
In our clinic, we frequently see patients whose HbA1c sits between 5.8% and 6.3% — technically prediabetic, but often dismissed as “borderline” elsewhere. When these patients commit to structured dietary changes and consistent physical activity, we regularly see HbA1c drop back below 5.7% within three to six months. The reversal is real, but it requires genuine commitment — not a two-week effort followed by a return to the old routine.
Why Prediabetes Develops
Prediabetes develops when the body’s ability to regulate blood sugar is gradually overwhelmed by a combination of genetic susceptibility, metabolic stress, and lifestyle factors. No single cause explains it — rather, it is the result of several forces working together over years.
Insulin resistance
The central driver is insulin resistance — a state where cells in the muscles, liver, and fat tissue respond less effectively to insulin. The pancreas compensates by producing more insulin, but this compensatory mechanism has limits. As insulin resistance worsens, blood sugar rises. South Asians appear to develop insulin resistance at lower BMI thresholds than Western populations, which is why prediabetes can affect people who do not appear overweight by conventional standards.
Visceral fat and abdominal obesity
Excess fat stored around the abdominal organs (visceral fat) is more metabolically active and inflammatory than subcutaneous fat. It directly impairs insulin signalling. This is why waist circumference is often a better predictor of metabolic risk than overall weight. For Indian men, a waist circumference above 90 cm, and for Indian women, above 80 cm, is considered elevated risk — lower thresholds than Western guidelines suggest.
Dietary patterns
A diet high in refined carbohydrates and low in fibre accelerates insulin resistance. In the Indian context, this often looks like heavy reliance on white rice, maida-based products (naan, biscuits, white bread), chai with multiple spoons of sugar, and frequent consumption of sweetened beverages and packaged snacks. Festival eating patterns — where concentrated sugar and refined-flour sweets are consumed over several days — can produce significant glycaemic spikes.
Physical inactivity
Sedentary behaviour reduces the muscles’ ability to absorb glucose efficiently. Regular physical activity — even moderate walking — directly improves insulin sensitivity. The inverse is also true: prolonged sitting worsens it.
Genetics and family history
A first-degree relative with type 2 diabetes significantly increases prediabetes risk. South Asian populations carry a higher genetic predisposition to insulin resistance and diabetes, which is part of why India’s prediabetes prevalence is so high even among younger and leaner individuals.
Sleep, stress, and other contributors
Chronic sleep deprivation (below 6 hours consistently), elevated cortisol from chronic stress, and conditions like polycystic ovary syndrome (PCOS) all independently contribute to insulin resistance and can accelerate the progression from normal glucose tolerance to prediabetes.
Tests and Ranges to Know
The three standard tests for identifying prediabetes are fasting plasma glucose, HbA1c, and the oral glucose tolerance test (OGTT). Each measures a different aspect of blood sugar regulation, and no single test tells the complete story.
Fasting plasma glucose (FPG) measures blood sugar after an 8–12 hour fast. A result between 100 and 125 mg/dL indicates prediabetes. It is the most commonly ordered test in routine check-ups, but it can miss patients whose blood sugar is normal in the morning yet spikes significantly after meals.
HbA1c reflects average blood sugar over the previous two to three months. A value between 5.7% and 6.4% falls in the prediabetic range. It does not require fasting, making it convenient, but can be affected by anaemia, haemoglobin variants, and recent blood loss — conditions that are not uncommon in India.
Oral glucose tolerance test (OGTT) measures blood sugar two hours after consuming a 75-gram glucose solution. A reading between 140 and 199 mg/dL indicates prediabetes. The OGTT is the most sensitive of the three for detecting early glucose intolerance, but it is less frequently ordered because it takes longer.
In our experience, relying on fasting glucose alone often misses the early stages of metabolic dysfunction. We frequently see patients whose fasting sugar is 95–99 mg/dL — technically “normal” — but whose OGTT or post-meal glucose tells a very different story. A fasting insulin level, while not part of the standard prediabetes definition, can also reveal compensatory hyperinsulinaemia — the body working overtime to keep blood sugar in range — long before glucose-based tests become abnormal.
The Most Effective Lifestyle Changes
Structured lifestyle modification — combining dietary changes, physical activity, and weight management — is the single most effective intervention for reversing prediabetes. This is not a general wellness recommendation; it is the conclusion of multiple large-scale randomised trials across different populations.
Weight loss: the single strongest lever
Losing 5–7% of body weight is the most impactful change a person with prediabetes can make. For someone weighing 80 kg, that means a loss of 4–5.6 kg. This level of weight reduction has been shown to substantially improve insulin sensitivity, lower fasting glucose, and reduce diabetes incidence. The DPP achieved its 58% risk reduction primarily through weight loss combined with activity. Importantly, this does not require dramatic dieting — moderate, sustained caloric reduction is more effective than aggressive short-term restriction followed by regain.
Physical activity: 150 minutes per week
A minimum of 150 minutes of moderate-intensity physical activity per week — the equivalent of a brisk 30-minute walk five days a week — significantly improves insulin sensitivity. Resistance training (bodyweight exercises, light weights) adds additional benefit by increasing the muscle tissue available to absorb glucose. Even a 10–15 minute walk after meals can meaningfully reduce post-meal glucose spikes.
Dietary changes: what matters most
Rather than following a single named diet, the most sustainable approach focuses on a few key principles:
- Reduce refined carbohydrates. White rice, maida products (naan, biscuits, white bread), and sugary snacks cause rapid blood sugar spikes. Replacing a portion of white rice with dal, vegetables, or millets like ragi and bajra can meaningfully lower the glycaemic load of a typical Indian meal.
- Increase fibre and protein. Whole dal, paneer, eggs, curd, nuts, and leafy vegetables slow glucose absorption and improve satiety. Starting a meal with vegetables or dal before rice can reduce the overall glucose spike.
- Limit liquid sugars. Sweet tea with 2–3 spoons of sugar consumed multiple times a day, packaged fruit juices, and sweetened lassi contribute a significant hidden sugar load. Switching to unsweetened chai or reducing to half a spoon makes a measurable difference.
- Watch portion sizes. A balanced Indian plate for metabolic health is roughly half vegetables, a quarter protein (dal, paneer, chicken, eggs), and a quarter complex carbohydrates — not the carbohydrate-dominant ratio many Indian meals default to.
Sleep and stress management
Chronic sleep deprivation and high cortisol directly worsen insulin resistance. Aiming for 7–8 hours of sleep, reducing screen exposure before bed, and addressing sleep apnoea if present are practical steps that support metabolic improvement. Stress management does not require meditation retreats — even consistent, brief daily walks, breathing exercises, or simply protecting adequate rest time can help lower cortisol.
How Long Reversal Can Take
Most patients who commit to consistent lifestyle changes begin seeing measurable improvement in blood sugar markers within 3–6 months, though individual timelines vary. HbA1c reflects a rolling 2–3 month average, so a retest sooner than 3 months may not capture the full effect of recent changes.
In the DPP trial, significant reductions in diabetes incidence were evident within the first year. The IDPP-1 tracked participants over 30 months, with benefits appearing within the first year for those who adhered to lifestyle recommendations. Real-world timelines depend on several factors:
- Starting HbA1c: A patient at 5.8% typically reverts to normal faster than one at 6.3%.
- Degree of insulin resistance: If fasting insulin is very high, the metabolic backlog takes longer to clear.
- Consistency of changes: Intermittent effort produces intermittent results. Sustained daily habits — not heroic two-week bursts — drive reversal.
- Coexisting conditions: PCOS, sleep apnoea, or significant visceral fat may slow the response and require additional intervention.
We typically recheck HbA1c and fasting glucose at 3 months, then again at 6 months. If markers are improving, the programme continues. If progress has stalled despite genuine adherence, it may be time to consider adding medication support — not as a failure, but as a practical next step.
When Medication May Still Be Needed
Lifestyle changes are the first and most effective line of defence, but medication — most commonly metformin — may be appropriate for certain patients with prediabetes. This is not a substitute for lifestyle changes; it is an addition when lifestyle alone has not been sufficient, or when risk factors are particularly high.
The ADA’s Standards of Care recommend considering metformin for prediabetic patients who have a BMI of 35 or higher, are under 60 years of age, or have a history of gestational diabetes. The DPP showed that metformin reduced diabetes risk by 31% — meaningful, but less effective than the 58% reduction achieved through lifestyle changes. In the Indian context, the IDPP-1 found that metformin reduced diabetes risk by 26.4% in a population that was notably leaner than the American DPP cohort.
In our practice, we discuss metformin when a patient has been consistently following lifestyle changes for three to six months but their HbA1c remains in the upper prediabetic range (6.0–6.4%), particularly if they have additional risk factors like a strong family history of diabetes, PCOS, or significant visceral adiposity. The decision is always made collaboratively — medication works best when it supports a lifestyle programme, not when it replaces one.
Newer agents like GLP-1 receptor agonists (e.g., liraglutide, semaglutide) have also shown efficacy in diabetes prevention, but their use in prediabetes is not yet standard practice and involves cost and access considerations, especially in India. Your physician can advise whether they are worth exploring in your specific situation.
Frequently Asked Questions
Is prediabetes permanent?
No. Prediabetes is one of the most reversible metabolic conditions when addressed early. Multiple large clinical trials — including the DPP and IDPP-1 — have demonstrated that lifestyle changes can return blood sugar markers to the normal range. However, reversal requires sustained effort. Patients who revert to previous habits often see blood sugar rise again. Think of it as a condition you can resolve, not one you simply outgrow.
What HbA1c is considered prediabetes?
An HbA1c between 5.7% and 6.4% is classified as prediabetes by the American Diabetes Association. Below 5.7% is considered normal; 6.5% or above meets the diagnostic threshold for type 2 diabetes. However, these are population-level cutoffs — not everyone at 5.6% is metabolically safe, and not everyone at 5.8% is in immediate danger. Context matters, which is why a clinician should interpret HbA1c alongside fasting glucose, post-meal patterns, and clinical history.
Can walking lower prediabetes risk?
Yes. Regular walking — especially brisk walking for at least 150 minutes per week — has been shown to improve insulin sensitivity and lower blood sugar. The DPP used brisk walking as its primary physical activity recommendation, and it contributed significantly to the 58% risk reduction observed. Even short post-meal walks of 10–15 minutes can help reduce post-meal glucose spikes. Walking is one of the most accessible and sustainable forms of exercise, particularly in the Indian context where gym access may be limited.
Can thin people get prediabetes?
Yes — and this is especially relevant in South Asian populations. Indian individuals tend to develop insulin resistance at lower body mass indices than Western populations, partly due to higher visceral fat distribution relative to overall weight. The IDPP-1 study participants had a mean BMI of just 25.8 kg/m², far below the DPP’s average of 34 kg/m², yet still had significant rates of glucose intolerance. A person can appear lean and still carry enough visceral fat to drive metabolic dysfunction. This is why waist circumference and metabolic blood work matter more than the bathroom scale alone.
| Take the Next Step If your blood sugar has been called “borderline” or “slightly elevated,” that is not a cue to wait — it is a cue to act. Prediabetes responds best to early intervention, and a structured metabolic assessment can reveal whether lifestyle changes alone are likely to be enough or whether additional support would help. Book an early-intervention consultation with our team at Redial Clinic, Green Park Extension, New Delhi, and find out exactly where you stand — and what you can do about it. |
References
- Diabetes Prevention Program Research Group, “The Diabetes Prevention Program (DPP): Description of lifestyle intervention,” Diabetes Care, 2002. https://doi.org/10.2337/diacare.25.12.2165
- Ramachandran A, Snehalatha C, Mary S, et al., “The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1),” Diabetologia, 2006. https://doi.org/10.1007/s00125-005-0097-z
- Crandall JP, Dabelea D, Knowler WC, et al., “The Diabetes Prevention Program and Its Outcomes Study: NIDDK’s Journey Into the Prevention of Type 2 Diabetes and Its Public Health Impact,” Diabetes Care, 2025. https://doi.org/10.2337/dc25-0014
- Anjana RM, Pradeepa R, et al., “Metabolic non-communicable disease health report of India: the ICMR-INDIAB national cross-sectional study (ICMR-INDIAB-17),” Lancet Diabetes Endocrinol, 2023. https://doi.org/10.1016/S2213-8587(23)00119-5
- American Diabetes Association, “Standards of Care in Diabetes — 2025: Prevention or Delay of Diabetes and Associated Comorbidities,” Diabetes Care, 2025. https://diabetesjournals.org/care/issue/48/Supplement_1
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before making changes to your diet, exercise, medication, or treatment plan.