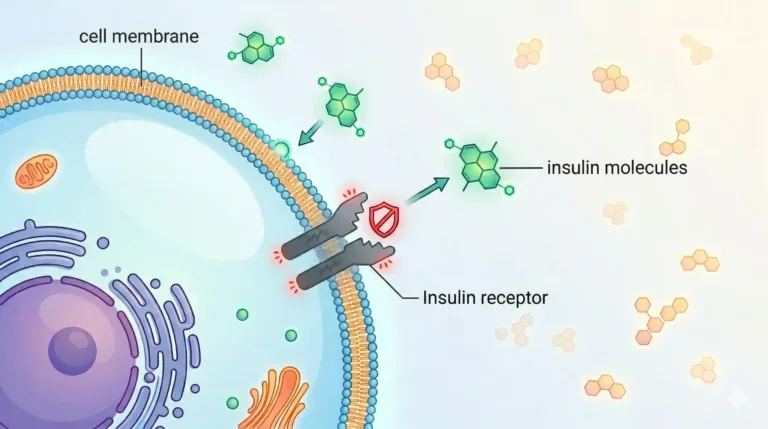
What does "diabetes reversal" actually mean?
Diabetes reversal, clinically called remission, is when HbA1c stays below 6.5% for at least three months without any glucose-lowering medication. It does not mean diabetes is gone forever. It means the metabolic conditions that were driving high glucose have been corrected enough that medication is no longer needed to keep sugar in a safe range.
This is the definition used by the American Diabetes Association, international consensus statements, and most serious reversal programs globally. We use it too.
Three important things follow from that definition:
Remission is real, measurable, and maintainable — but it is not permanent by default. It requires continued attention to the underlying drivers.
Remission requires medication-free glucose control. If you are in the normal range only because metformin or insulin is working, that is well-controlled diabetes, not reversal. Both are valuable. They are not the same thing.
Remission depends on when in the disease you act. Early action — especially in the first 6 years after diagnosis — carries a higher probability of sustained remission than intervention after 15+ years.
Can type 2 diabetes be reversed?
Yes, for many people with type 2 diabetes, structured metabolic treatment can achieve remission — particularly when the diagnosis is recent, insulin reserve is preserved, and excess visceral fat can be reduced. The DiRECT trial published in Lancet in 2018 showed 46% of participants achieved remission at 12 months with structured weight-loss intervention, rising to 86% among those who lost 15 kg or more.
Whether an individual patient can achieve remission depends on several measurable factors: how long you have had diabetes, your current beta-cell reserve, the degree of insulin resistance, the amount of visceral fat, current medication regimen, and your readiness to make meaningful changes under medical supervision. The honest answer is that some patients can, some cannot, and the purpose of an initial assessment is to tell the difference clearly — not to sell a guarantee.
What is more broadly true is that almost every patient with type 2 diabetes can improve substantially with the right treatment architecture, even when full remission is not achievable. HbA1c comes down, insulin sensitivity recovers measurably, cardiovascular risk drops, and medication requirements often reduce — even when the diabetes label stays.
How long does it take to reverse type 2 diabetes?
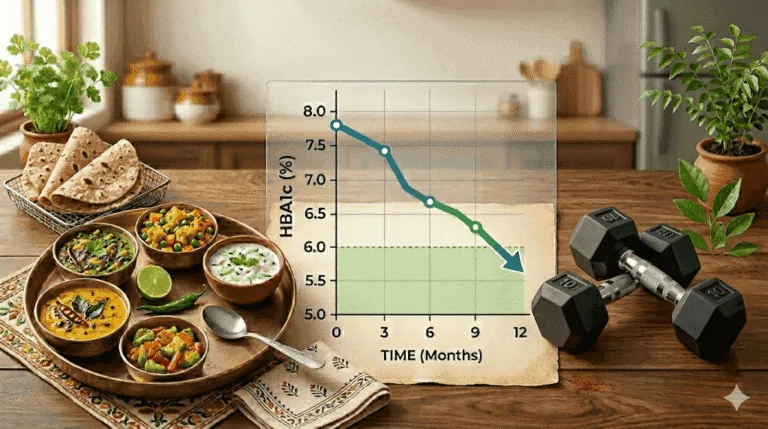
For suitable patients, early glucose improvements typically appear within 4 to 8 weeks of structured treatment. HbA1c — which reflects the previous 3 months of glucose — usually shows meaningful reduction by 3 months and may reach remission thresholds between 6 and 12 months. Full durable remission, where medication has been successfully discontinued and HbA1c stays below 6.5%, typically takes 6 to 18 months of consistent work.
These are population averages, not guarantees. Individual timelines depend on starting HbA1c, insulin reserve, duration of diabetes, current medications, and how consistently the treatment plan is followed. A patient diagnosed within the last 2 years with moderate HbA1c elevation usually progresses faster than a patient with 12 years of diabetes and significant complications. The initial assessment lets us give you an honest timeline based on your data, not a brochure average.
Typical progression in suitable patients
- Weeks 2–6: Improved daily energy, reduced post-meal crashes, lower fasting glucose, fewer hypoglycaemic episodes in medicated patients (often requiring early medication review).
- Months 2–4: Measurable fat loss, improved body composition, lower HbA1c on repeat testing, early supervised medication reduction in suitable candidates.
- Months 3–6: Significant HbA1c improvement, often approaching or crossing remission threshold; further medication reduction where clinically appropriate.
- Months 6–18: Durable remission in suitable patients; patient is medication-free with HbA1c <6.5% sustained for 3+ months.
- Beyond 18 months: Maintenance phase — periodic monitoring, lifestyle consolidation, early detection of any relapse signals.
What You Can Expect at Redial
Every diabetes reversal program at Redial is built on four principles that distinguish doctor-led metabolic care from app-based protocols.
Diagnostic Depth
Indian Clinical Context
Continuity of Care
Honest Expectations
Can diabetes complications be reversed?
Some diabetes complications can be partially or substantially reversed with sustained glucose normalisation; others can only be halted or slowed, not undone. Early neuropathy and early diabetic kidney damage show the most potential for improvement. Established retinopathy and advanced nerve damage are harder to reverse but can usually be stabilised. Honest assessment of where you are on this spectrum matters more than promises.
Diabetic neuropathy
Early peripheral neuropathy — tingling, mild numbness, burning sensations in the feet — can improve meaningfully with sustained glucose normalisation, weight reduction, and correction of nutritional deficiencies (particularly B12 in patients on long-term metformin). Established, advanced neuropathy with significant nerve damage usually stabilises or progresses more slowly but does not fully reverse. The window to improve neuropathy is real but narrows with time.
Diabetic kidney damage (diabetic nephropathy)
Early-stage diabetic kidney disease — detected by elevated urine albumin or mildly reduced eGFR — can often stabilise or improve with aggressive glucose control, blood pressure management, and appropriate medication (including SGLT2 inhibitors where indicated). Moderate-to-advanced kidney disease typically cannot be reversed but progression can be slowed significantly. Catching kidney involvement early — which requires looking for it, not waiting for symptoms — changes the trajectory.
Diabetic retinopathy
Retinopathy is largely structural damage to retinal blood vessels. Once established, it cannot be “reversed” in the everyday sense — but its progression can be halted and in some cases partially stabilised with glucose normalisation, blood pressure control, and ophthalmology-led treatment where indicated. Preventing further damage is the realistic goal for most patients with existing retinopathy.
Diabetic foot complications
Foot ulcers, infections, and peripheral vascular disease are serious complications that require coordinated care with vascular and podiatric specialists. Once tissue damage has occurred, full reversal is often not possible, but further risk can be reduced substantially through glucose control, vascular support, and careful foot care protocols.
What we actually assess — and why it differs from most clinics
A standard diabetes workup in India typically looks at fasting glucose, HbA1c, and a lipid panel. That is useful but partial. We additionally assess fasting insulin, HOMA-IR, body composition, liver function relevant to metabolic health, a complete lipid subfraction where indicated, and the daily inputs — food, sleep, movement, stress — that drive your glucose patterns. Diagnostic depth is how we avoid treating the wrong problem.
The assessment covers:
How the diabetes reversal program works
The program is built around four clinically validated levers: nutrition correction structured around real Indian food, strength and movement work that rebuilds muscle-driven glucose uptake, sleep and stress correction that reduces cortisol-driven insulin resistance, and a supervised medication review that reduces drug burden when glucose responses make it clinically safe to do so.
Diet — the primary metabolic lever
Three structured meals with no snacking between them — because every time you eat, insulin rises, and reversal requires insulin to fall between meals. A real protein source at every meal (eggs, paneer, curd, chicken, fish — dal alone is not enough), controlled carbohydrate portions over refined ones, and ghee replacing inflammatory seed oils. The food is Indian: eggs, paneer, moong dal, ghee-cooked sabzis. Nothing exotic, nothing imported.
Strength and movement
Muscle is where most glucose is disposed of. Building or preserving muscle mass is a core part of reversal, not an optional lifestyle add-on. We work with what you can actually sustain — sometimes structured resistance training, sometimes walking and functional work, always calibrated to your current fitness and any complications.
Sleep, stress, and metabolic load
Poor sleep and chronic stress drive cortisol, which worsens insulin resistance directly. Most patients do not realise how much of their glucose problem is downstream of under-slept nights and unmanaged stress. Addressing this is not soft medicine — it is metabolic medicine.
Supervised medication review
As glucose responses improve, medication doses can often be reduced. This must be done under supervision, never independently. We track glucose response carefully and reduce medication when — and only when — the data supports it. Some patients reach full medication discontinuation; others reduce doses but continue on modified regimens. Both outcomes are legitimate.
Diabetes in the Indian patient — why South Asian context matters
India is home to an estimated 101 million people with diabetes and 136 million with prediabetes, according to the ICMR-INDIAB study published in Lancet Diabetes & Endocrinology in 2023. Indian patients also develop type 2 diabetes at lower BMI and younger ages than European or American populations — a pattern driven by the South Asian metabolic phenotype: higher visceral fat, lower muscle mass, earlier beta-cell dysfunction. Treatment approaches imported without adjustment consistently underperform in this population.
Three specific points where Indian context changes the work:
- BMI thresholds are different. ICMR considers BMI ≥23 kg/m² as overweight and ≥25 kg/m² as obese in Indian adults — substantially lower than WHO global cutoffs. A patient with BMI 26 may be told they are ‘only slightly overweight’ by Western standards while actually being obese by Indian guidelines.
- Waist circumference matters more than total weight. Central adiposity — visceral fat around the abdomen — is the metabolically relevant marker in South Asian patients, with thresholds of ≥90 cm for men and ≥80 cm for women flagging elevated risk.
- Nutrition corrections must fit Indian food. A plan built around oats, broccoli, and salmon fails in Indian kitchens, at Indian restaurants, and at Indian family gatherings. Reversal-capable nutrition has to work with dal, rice, roti, sabzi, chai, and festival eating, not against them.
The breakfast problem: Poha, upma, idli, and toast — the standard Indian breakfast — are carbohydrate-dominant and contain almost no protein. Blood sugar spikes, insulin rises, and the patient is hungry and snacking before 11 AM. Switching breakfast to a protein-first meal is consistently one of the highest-impact single changes in Indian T2DM management.
Chai with sugar is the most common hidden glycaemic load: Three cups daily with two teaspoons of sugar each = 25 grams of added sugar before a single meal. Most patients do not count this. Auditing and reducing chai sugar alone often produces measurable HbA1c improvement within eight weeks.
Dal is not enough protein: One katori of dal provides 8–9 grams of protein. A meal needs 25–30 grams to manage glucose, reduce hunger, and support muscle. The gap — present at every meal in most Indian diets — keeps patients insulin-resistant and hungry. It must be filled by eggs, paneer, curd, fish, or chicken alongside the dal, not instead of it.
Cooking oil is rarely addressed — and it should be: Sunflower and refined vegetable oils, used daily in large quantities in Indian cooking, are high in omega-6 fatty acids that drive systemic inflammation and worsen insulin resistance. Switching to ghee as the primary cooking fat addresses this at the root.
Who this program is for — and who it is not for
This program is designed for
- Adults with type 2 diabetes or prediabetes who want a clinically serious treatment plan, not another round of vague lifestyle advice
- Patients diagnosed within the last 1–10 years who still have meaningful beta-cell reserve
- Patients with HbA1c in the 5.7–8.5% range with preserved insulin reserve — the group with the highest reversal probability
- Patients whose medication burden is increasing year over year and want a different trajectory
- Patients with fatty liver, high waist circumference, or a strong family history of diabetes looking for upstream prevention
This program is not designed for
- Type 1 diabetes — an autoimmune condition requiring lifelong insulin, not addressable through metabolic reversal
- Patients unwilling to change food patterns, activity, or sleep — reversal requires behavioural change, not just clinical oversight
- Patients expecting a quick fix or guaranteed cure — we work seriously, not theatrically
Why patients choose Redial over hospital, diabetes clinics, and app-based programs
Hospital diabetes clinics in Delhi are optimised for medication titration and acute care, not reversal. App-based programs are optimised for scale, not clinical depth. Redial occupies the space in between: a doctor-led, small-scale clinic practising metabolic medicine with proper diagnostic depth, direct physician involvement, and Indian-context nutrition — delivered in person at our Green Park Extension clinic in New Delhi, with hybrid follow-up available.
- Doctor-led, not app-led. Every treatment plan is built and reviewed by a metabolic-medicine physician, not a chatbot or a standardised protocol.
- Diagnostic depth. We look at fasting insulin, HOMA-IR, body composition, and the markers that actually drive reversal — not just the basic panel.
- Indian clinical context. ICMR thresholds, South Asian phenotype, Indian dietary patterns — built into the work, not bolted on.
- Honest expectations. We tell you what reversal probability looks like for your specific case, including when it does not apply. No guaranteed outcomes, no miracle claims.
- Continuity. Same clinician across your journey. You are not rotated through a care team.