What is PCOS, really?
PCOS (Polycystic Ovary Syndrome) is a metabolic-hormonal condition affecting an estimated 1 in 5 Indian women of reproductive age. It is diagnosed by the Rotterdam criteria: two of three features — irregular or absent ovulation, clinical or biochemical signs of elevated androgens (acne, facial hair, elevated testosterone), and polycystic ovaries on ultrasound. It is not primarily an ovarian problem. It is a whole-body syndrome in which insulin resistance and androgen excess drive most of what the patient experiences.
The common presentations include:
- Irregular, infrequent, or absent menstrual periods
- Acne, oily skin, and excess facial or body hair (hirsutism)
- Scalp hair thinning or male-pattern hair loss
- Difficulty conceiving or irregular ovulation
- Weight gain, particularly around the abdomen, and resistance to weight loss
- Darkened skin patches (acanthosis nigricans) on the neck, underarms, or groin — a sign of insulin resistance
- Mood changes, anxiety, and fatigue — all more common in PCOS than in controls
PCOD vs PCOS — what is the actual difference?
PCOD (Polycystic Ovarian Disease) and PCOS (Polycystic Ovary Syndrome) are often used interchangeably in India, but they refer to different things. PCOD describes the ultrasound finding of multiple small cysts on the ovaries, which can occur in otherwise healthy women. PCOS is a clinical syndrome — a diagnosis that requires at least two of: irregular ovulation, signs of elevated androgens, and polycystic ovaries on imaging. Every woman with PCOS has some ovarian changes, but not every woman with polycystic ovaries has PCOS.
The practical distinction matters because treatment implications differ:
- A woman with polycystic ovaries on scan but regular periods, normal androgens, and no other symptoms has PCOD appearance — not PCOS. She may need no specific treatment.
- A woman with irregular periods, acne, facial hair, and insulin resistance — even with normal-looking ovaries on scan — can still have PCOS. The ultrasound is one criterion among three, not the defining one.
- In everyday Indian clinical conversation, ‘PCOD’ is often used to mean ‘PCOS’ informally. This leads to patients being told ‘you have PCOD, here are some pills’ without a proper PCOS workup. The result is undertreatment of a real metabolic syndrome.
Can PCOS be cured?
PCOS cannot be cured in the sense that it is permanently gone with no possibility of return — the underlying genetic and metabolic susceptibility remains. But PCOS can be managed extremely well, and for many women, the symptoms that bring them to the clinic — irregular periods, acne, weight gain resistance, elevated androgens, difficulty conceiving — can be substantially or fully reversed with sustained treatment. “Cure” is the wrong word; “remission” and “sustained control” are the right ones.
What meaningful PCOS remission looks like in practice:
- Regular or near-regular menstrual cycles restored
- Significant reduction in androgen-driven symptoms (acne, facial hair, hair loss)
- Improved insulin sensitivity and metabolic markers
- Weight stabilisation or meaningful weight reduction where relevant
- Restoration of ovulation in women seeking fertility
- Reduced need for hormonal or metabolic medication over time, in suitable patients
This outcome is real and achievable for a meaningful proportion of patients, but it is not automatic and it is not permanent by default. PCOS remission requires sustained attention to the drivers — primarily insulin resistance and body composition — rather than a finite course of pills. Anyone offering a 3-month ‘cure’ is either misunderstanding the condition or overselling.
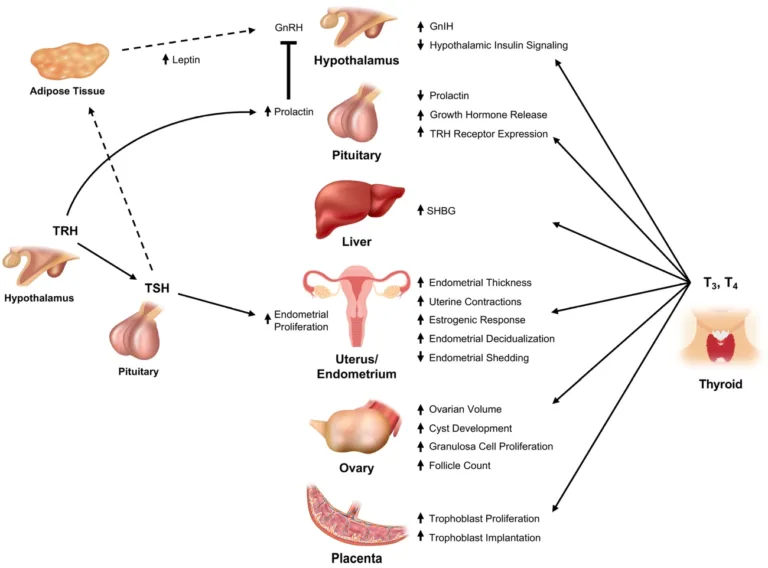
The metabolic driver — why insulin resistance is central to PCOS
Insulin resistance is present in 50–70% of women with PCOS, including many who are not overweight. Excess insulin directly stimulates the ovaries to produce more androgens and reduces the liver’s production of sex hormone binding globulin, raising the level of free (biologically active) testosterone. The result is the cascade that PCOS patients actually experience: androgen excess, disrupted ovulation, irregular periods, weight gain, and worsening metabolic markers. Treating PCOS without addressing insulin resistance is treating the symptoms, not the driver.
Why this matters for treatment choice:
- Hormonal contraceptive pills regulate bleeding but do not correct the underlying insulin resistance — they mask the cycle problem while the metabolic drivers continue unchecked
- Metformin and insulin-sensitising nutrition directly address the upstream driver — they do less for acute period regulation but much more for long-term PCOS trajectory
- Combined approaches (addressing insulin resistance metabolically while using hormonal treatment where needed for specific symptoms) usually outperform either approach alone
- Inositol supplements, specifically myo-inositol combined with d-chiro-inositol, have clinical evidence for improving ovulation and insulin sensitivity in PCOS — they are a legitimate option to discuss, not a magic bullet
The dietary response to insulin resistance is specific, not vague. Three structured meals with no snacking between them is the most important behavioural change — not because of calories, but because every time you eat, insulin rises. Fat burning and insulin sensitisation both require insulin to fall between meals. The Indian habit of eating small amounts frequently throughout the day, which feels like moderation, keeps insulin elevated and reinforces the PCOS cycle.
The foods that directly worsen insulin resistance in PCOS: white rice in large portions, maida products (bread, biscuits, paratha), packaged snacks, fruit juice, chai with sugar, and flavoured dairy. The foods that support insulin correction: eggs and paneer at breakfast (protein-first mornings stabilise blood sugar through the most insulin-sensitive part of the day), full-fat plain curd, moong dal, leafy greens, and ghee as the cooking fat over inflammatory seed oils.
Lean PCOS — yes, you can have PCOS without being overweight
Lean PCOS refers to women who meet PCOS diagnostic criteria but have BMI in the normal or low range — roughly 20–30% of women with PCOS fall into this category. Insulin resistance is still commonly present despite normal weight, often driven by central (visceral) fat distribution, muscle mass relative to fat mass, or genetic factors. Lean PCOS is regularly underdiagnosed because patients and clinicians both assume PCOS requires visible weight excess — it does not.
Common patterns we see in lean PCOS:
- Patient with BMI 20–23 but a waist circumference that suggests central adiposity relative to her frame
- Irregular periods dismissed as stress or lifestyle rather than investigated
- Acne and mild facial hair attributed to genetics rather than recognised as androgen excess
- Normal fasting glucose and HbA1c but elevated fasting insulin, pointing to early insulin resistance
- Fertility difficulty that prompts the first real diagnostic workup — often years after symptoms began
Lean PCOS still responds to metabolic-first treatment: insulin-sensitising nutrition, strength training to build muscle-driven glucose disposal, adequate sleep and stress management, and — where indicated — insulin sensitisers or hormonal support. The weight is not the problem; the metabolic biology is.
What we actually assess — a full PCOS workup
A proper PCOS workup goes beyond a hormonal panel and an ultrasound. We additionally assess fasting insulin and HOMA-IR, complete lipid profile, liver markers (fatty liver is strongly linked to PCOS), thyroid function, body composition, and where clinically relevant, adrenal hormones to exclude other androgen-excess causes. The goal is to establish the full metabolic and hormonal picture, not just confirm the diagnosis.
How the PCOS program works
The program runs on four connected tracks: insulin-sensitising nutrition structured for Indian food, strength and movement work to improve insulin sensitivity through muscle, sleep and stress correction as genuine metabolic levers, and medical care — including hormonal treatment, metformin, inositol, or other medications where clinically appropriate. Where fertility is part of the goal, we coordinate with gynaecology rather than replacing their care.
Nutrition — insulin-sensitising, Indian-food-centric
Three structured meals with no snacking — every meal raises insulin, and PCOS responds directly to insulin control. Protein at every meal: eggs, paneer, curd. Full-fat dairy over skim or flavoured. Ghee as the cooking fat. Spearmint tea daily for its documented mild anti-androgenic effect. Built around Indian food — nothing exotic, nothing that requires a separate kitchen.
Strength and movement
Muscle is where most glucose is disposed of, and women with PCOS who prioritise strength training typically see meaningful insulin sensitivity improvement. Resistance training, progressive loading calibrated to the patient’s current fitness, walking, and functional movement form the movement workstream. Cardio alone — the default PCOS advice — does less for insulin resistance than properly programmed strength work.
Sleep, stress, and androgens
Chronic poor sleep raises cortisol, which worsens insulin resistance and disrupts reproductive hormones. Chronic stress does the same. Addressing both is not soft medicine — it is metabolic medicine with measurable hormonal effects. For many patients, this is the hardest but highest-yield work.
Medical care — coordinated with gynaecology where needed
Depending on the presentation, treatment may include metformin for insulin resistance, inositol supplementation for ovulation and insulin sensitivity support, hormonal contraceptive options for cycle regulation and androgen control where appropriate, spironolactone or other anti-androgen therapy for significant hirsutism or acne, or targeted fertility medications (coordinated with gynaecology). We are not ideological about medications — we discuss them openly where they can help.
PCOS and fertility — what to know if you are trying to conceive
PCOS is one of the most common causes of female-factor infertility in India, but it is also among the most treatable. The underlying problem is usually anovulation — the ovaries not releasing an egg regularly — driven by insulin resistance and androgen excess. Many women with PCOS conceive without fertility medication once the metabolic drivers are addressed. Others benefit from ovulation induction or assisted reproduction, coordinated with a gynaecologist. Our role is the metabolic foundation that makes fertility treatment more likely to succeed.
What we focus on when a patient with PCOS is trying to conceive:
- Correcting insulin resistance before and during ovulation induction — outcomes of fertility treatment are substantially better when insulin sensitivity is improved
- Body composition optimisation where BMI is elevated — even 5–10% weight reduction can restore ovulation in many women
- Metformin or inositol support where indicated to improve ovulation frequency
- Coordinating with gynaecology when ovulation induction (letrozole, clomiphene) or assisted reproduction is part of the plan
- Continuing metabolic care through pregnancy and postpartum — PCOS increases risk of gestational diabetes and pregnancy complications, which are modifiable with proper oversight
Important: we do not replace gynaecology care, perform fertility procedures, or issue fertility-specific prescriptions that are properly gynaecologist territory. We handle the metabolic and endocrine foundation; fertility specialists handle the fertility procedures. Coordinated care works better than parallel separate care.
PCOS in Indian women — why context matters
PCOS prevalence in Indian women is estimated at approximately 1 in 5 in community-based studies, among the highest rates globally. Contributing factors include the South Asian metabolic phenotype (central fat distribution, earlier insulin resistance), modern lifestyle shifts (sedentary work, high refined-carbohydrate intake, disrupted sleep), and under-diagnosis leading to late-stage presentations. Indian women also face specific challenges in care — hormonal contraceptive resistance, family pressure around fertility timelines, and a cultural tendency to treat symptoms in isolation.
- ICMR and AIIMS-led Indian studies estimate PCOS prevalence at 10–22% of reproductive-age women, with substantial regional variation and likely under-diagnosis
- The South Asian metabolic phenotype amplifies insulin resistance at lower BMI — which is why lean PCOS is particularly common in Indian women
- Indian dietary patterns high in refined carbohydrates (white rice, maida, sugar, processed snacks) worsen insulin resistance — modifiable
- Cultural pressure around fertility timelines sometimes forces patients into fertility treatment before metabolic foundation work is done — a coordinated approach produces better outcomes
Who this program is for — and who it is not for
This program is designed for
- Women diagnosed with PCOS or PCOD who want a metabolic-first, integrated approach
- Women suspected to have PCOS but never properly worked up — irregular periods, acne, facial hair, weight difficulty, or family history
- Women with lean PCOS who have been dismissed with 'you don't look like PCOS'
- Women with PCOS planning pregnancy who want the metabolic foundation optimised before or alongside fertility care
- Adolescent girls and young women with PCOS-like symptoms, with appropriate family and paediatric coordination
- Women with PCOS plus other metabolic issues (diabetes, prediabetes, fatty liver, weight difficulty) who want them treated together
This program is not designed for
- Active fertility treatment or IVF — we provide the metabolic foundation; gynaecology and fertility specialists run fertility procedures
- Pregnancy care — obstetric care is gynaecologist territory; we can continue metabolic oversight in coordination
- Women expecting a quick fix or a 3-month 'cure' — we offer honest sustained improvement, not magic